A 32 year old female came to JIPMER, department of cardiology with history of palpitation since last 10 years, increased frequency since last 2 months, had two episode each lasting two to three hours, acute onset associated with giddiness, vomiting, chest pain, dyspnoea, and subsided on taking medication from local doctors.Patient ECG both during tachycardia and during sinus rhythm is shown below.ECHO heart was normal.
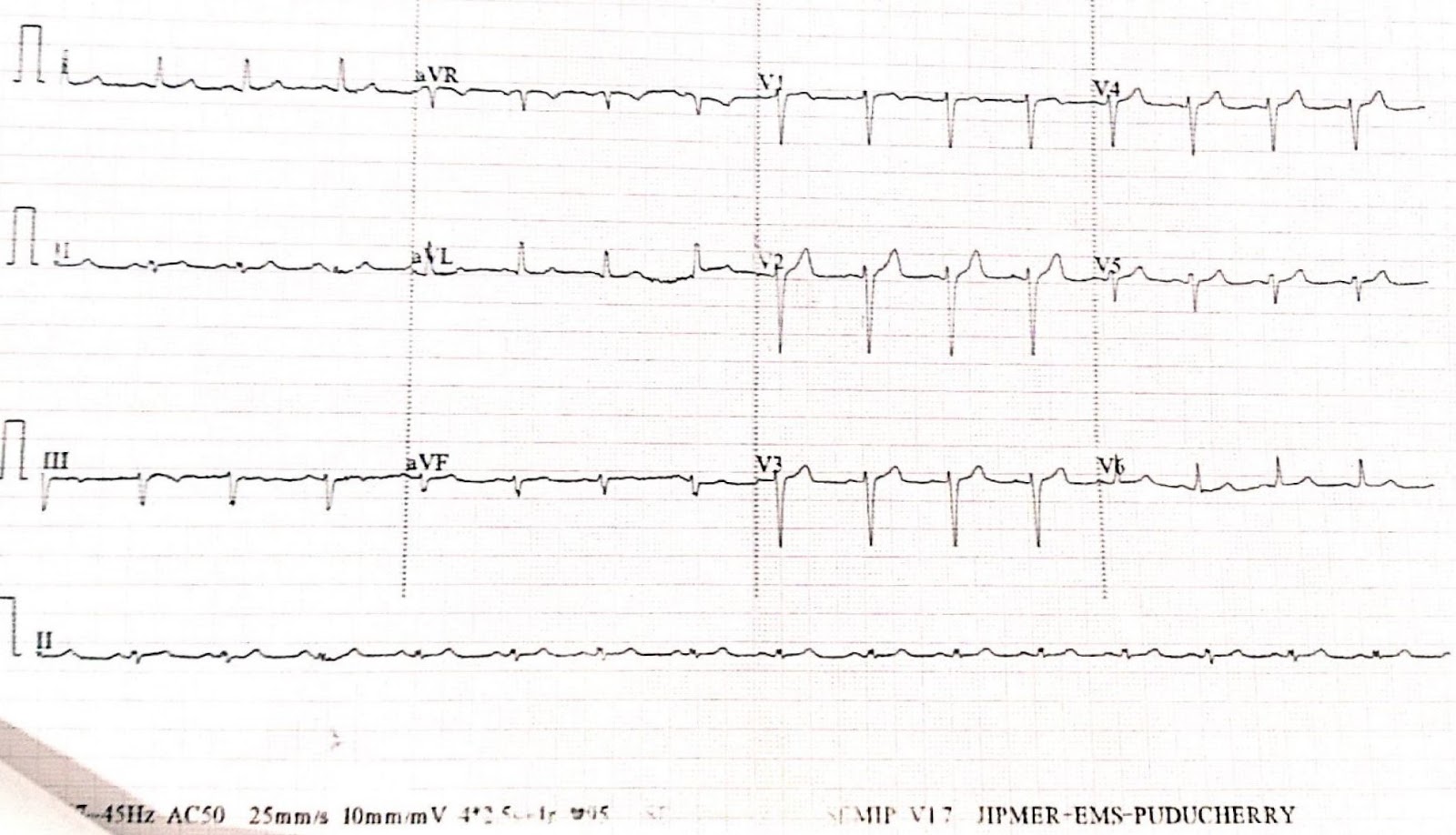
ECG during tachycardia
Description of the tachycardia ECG-Regular narrow complex tachycardia at rate 200 beats per minutes, LBBB morphology, QRS duration 120 msec, LAD, QRS duration nearly 120 msec, no AV dissociation, No P wave,No capture beat, no fusion beat
ECG during sinus rhythm
ECG description-Sinus rhythm at around 75 per minute, LAD, No ST-T wave changes, No evidence of pre-excitaion
Differential diagnosis- PSVT, SVT with aberrancy
SVT with pre-excitation, ?Mahaim fiber tachycardia
Ventricular tachycardia
Patient underwent Electrophysiological study at Department of Cardiology, JIPMER, Pondicherry, India, by Dr Raja Selvaraj and his team. It was suggestive of Antidromic reentrant tachycardia with mahaim accessory pathway. Patient underwent successful radiofrequency ablation.
UpToDate. Mahaim fiber tachycardias
INTRODUCTION — The term cardiac preexcitation was originally used to describe premature activation of the ventricles in patients with the Wolff-Parkinson-White (WPW) pattern. This term has been broadened to include all conditions in which antegrade ventricular activation or retrograde atrial activation occurs partially or totally via an anomalous pathway distinct from the normal cardiac conduction system.
The classic form of cardiac preexcitation is the WPW pattern, which is characterized by a short PR interval and a broad QRS complex with a delta wave. The anatomic substrate for this is a band of myocytes that bridges the fibrous atrioventricular junction, also known as the bundle of Kent . The electrocardiographic features are a result of premature ventricular activation due to conduction over the accessory pathway.
Several other pathways, such as Mahaim fibers, have been postulated to result in cardiac preexcitation. However, most lack the histopathologic correlation that has been demonstrated for the WPW pattern. This topic will discuss the Mahaim fiber tachycardias. WPW and other non-WPW forms of preexcitation are discussed separately.
ANATOMIC AND FUNCTIONAL FEATURES — In 1937, during pathologic examination of the heart, Mahaim and Benatt identified islands of conducting tissue extending from the His bundle tissue into the ventricular myocardium . These fibers were termed Mahaim or fasciculoventricular fibers . This description was subsequently expanded to include connections between the atrioventricular (AV) node and the ventricular myocardium (nodoventricular fibers) . These findings have been confirmed by other investigators, but true continuity of these pathways is less common than was initially suspected .
Mahaim fibers were originally classified into two main groups depending upon their site of origin :
- Nodoventricular fibers
- Fasciculoventricular fibers
This classification had a functional as well as an anatomic significance, since the two groups were thought to be associated with different clinical features . The nodoventricular connections were presumed responsible for the generation of an AV reentrant tachycardia (AVRT) with a left bundle branch block morphology that had unique electrophysiologic features . This arrhythmia was not seen in patients with fasciculoventricular fibers.
This classification for Mahaim fibers persisted until evidence suggested that the anatomic cause for the tachycardia with characteristics previously attributed to nodoventricular fibers is a slowly conducting AV accessory pathway with decremental conduction (ie, conduction slows at faster heart rates) . This accessory pathway, which only conducts in an antegrade fashion, most often arises in the anterior wall of the right atrium and inserts into the right ventricle, close to the right bundle branch.
These unusual accessory pathways are responsible for the constellation of electrophysiologic features that define Mahaim tachycardias. Histologic and functional examination of tissue from patients treated surgically has demonstrated an accessory pathway with features similar to normal atrioventricular nodal tissue. The presence of nodal tissue in the accessory pathway would account for the decremental properties seen in Mahaim fibers, which is not characteristic of other accessory pathways.
Two types of decremental right-sided accessory pathways, both arising from the tricuspid annulus but with different ventricular insertions, may be responsible for Mahaim tachycardia :
- Atriofascicular connections, which account for approximately 80 percent Mahaim fibers, have a long intracardiac course and insert into the distal right bundle or right ventricle near its apex, often with arborization. A possible morphologic and functional explanation for these connections, involving the moderator band, has been proposed.
- Atrioventricular pathways, accounting for approximately 20 percent of Mahaim fibers, insert proximally into the right ventricle near the atrioventricular annulus close to the conducting system .
The term Mahaim tachycardia describes the typical constellation of electrophysiologic features that characterize this unusual form of reentrant tachycardia, without implication as to the underlying anatomic cause.
ELECTROCARDIOGRAPHIC FEATURES — The resting electrocardiogram (ECG) in patients with Mahaim fibers is usually normal
In contrast to the WPW pattern, there is no delta wave with Mahaim fiber conduction. As noted above, the Mahaim pathways terminate in the ventricles into or near the conducting system; in contrast, insertion occurs into the ventricular myocardium, with slow muscle fiber-to-muscle fiber conduction in patients with the WPW pattern. It is this combination of preexcited and slowed conduction that is responsible for the delta wave.
There are several ECG features that suggest Mahaim fibers as the cause of a tachycardia with a left bundle branch block pattern These include:
- QRS axis between 0 and minus 75º
- QRS duration of 0.15 seconds or less
- R-wave in lead 1
- rS complex in lead V1
- Precordial transition in lead V4 or later
- Cycle length between 220 and 450 milliseconds (heart rates of 130 to 270)
Although these criteria are useful, they are not diagnostic of a Mahaim tachycardia.