A 50 year old male presenting with history of giddiness along with 3 episode of vomiting since 4 hours of duration. There was no history of chest pain, palpitation, sweating, syncope. Patient was non diabetic, non hypertensive. His pulse was 50 beats per minute, BP-110/70 mmhg during the time of admission. Patient ecg done in the emergency department is shown below.

ECG of the patient is showing complete AV dissociation with ST segment elevation in lead III, avF, but elevation was less than 1 mv......


ECG is showing ST segment elevation in lead III, very mild ST segment elevation in lead II, avF

ECG is showing ST segment elevation in lead II,III, avf, with hyperacute Tall T wave, now instead of complete AV block there is 4:3 type I 2nd degree AV block (Wenckebach block) with group beating present.

ECG is not showing any evidence of right sided infarction as there is absence of ST segment elevation in right sided lead.
Patient was immediately started on thrombolysis.

ECG is showing complete resolution of ST segment along with resolution of AV block. PR interval is although borderline prolonged, PR interval after thombolysis is 160 msec.

ECG become completely normal next day. There is no evidence of AV block, neither any evidence of ST segment elevation.
Next day patient underwent coronary angiography which shows 70-80% stenosis in Mid right coronary artery(RCA) rest of the vessel were normal.
So the final diagnosis of the patient is IWMI with complete heart block with successful thrombolysis with Single vessel diseases of RCA.
Thank you.
ECG 1 (Click on the image to enlarge it)

ECG of the patient is showing complete AV dissociation with ST segment elevation in lead III, avF, but elevation was less than 1 mv......
ECG 2 taken after 10 min

ECG is still showing same finding as in first ECG
ECG 3

ECG is showing ST segment elevation in lead III, very mild ST segment elevation in lead II, avF
ECG 4 done after 30 min

ECG is showing ST segment elevation in lead II,III, avf, with hyperacute Tall T wave, now instead of complete AV block there is 4:3 type I 2nd degree AV block (Wenckebach block) with group beating present.
ECG with right sided lead
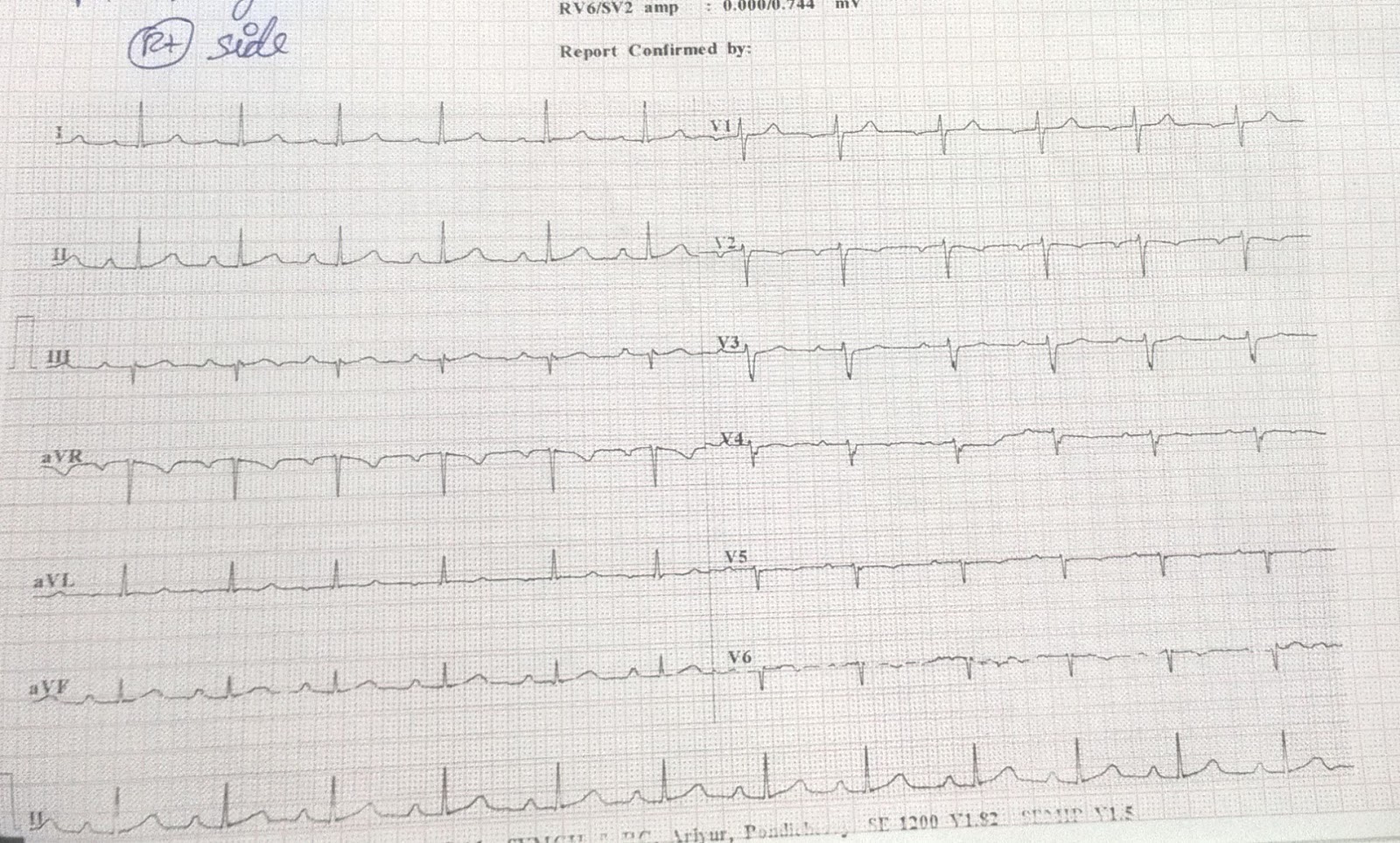
ECG is not showing any evidence of right sided infarction as there is absence of ST segment elevation in right sided lead.
Patient was immediately started on thrombolysis.
Post thrombolysis ECG is shown below
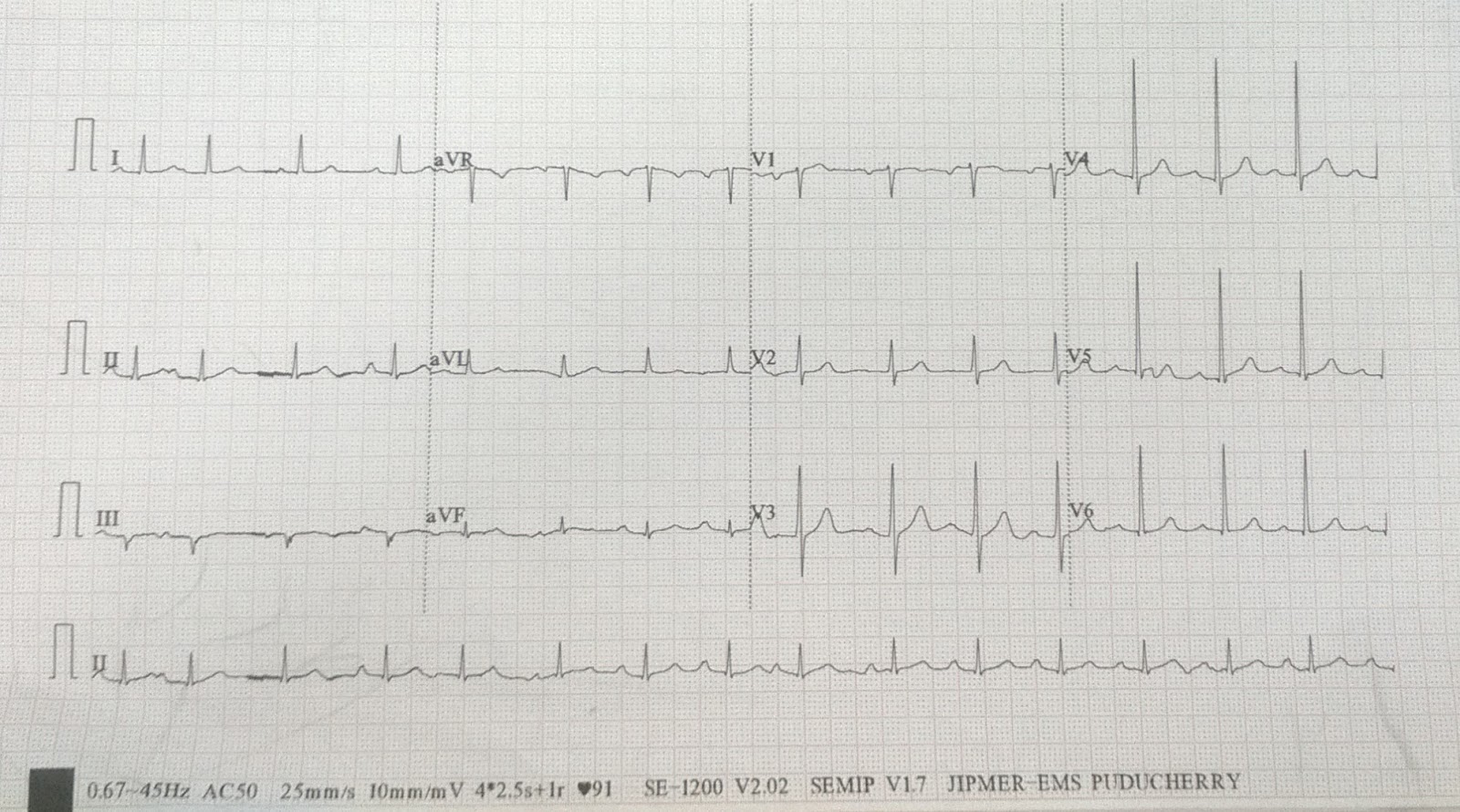
ECG is showing complete resolution of ST segment along with resolution of AV block. PR interval is although borderline prolonged, PR interval after thombolysis is 160 msec.
ECG done next day

ECG become completely normal next day. There is no evidence of AV block, neither any evidence of ST segment elevation.
Next day patient underwent coronary angiography which shows 70-80% stenosis in Mid right coronary artery(RCA) rest of the vessel were normal.
So the final diagnosis of the patient is IWMI with complete heart block with successful thrombolysis with Single vessel diseases of RCA.
Thank you.
No comments:
Post a Comment