A 49 years old male with a known case of Ostium secundum atrial septal defect with bidirectional shunt with Eisenmenger syndrome come to the JIPMER emergency department with chief complaints of palpitation since today morning which were acute in onset, patient went to private hospital, ECG done and DC cardioversion done. Tachycardia subsided but again started after 10 minute so patient was referred to JIPMER hospital for further management. Patient on inquiry was giving history of similar palpitation on and off since last 2 months, which were acute in onset, remain for 30 minutes and subsided on its own. During evaluation in the emergency department patient pulse rate was 200 beats per minute, Blood pressure was 100/56 mm hg, was complaining of dyspnoea of NYHA class III. On examination CVS S1S2 present, S2 was loud. RS-B/L normal vesicular breath sound, there was no crepitation. DC cardioversion done in view of dyspnoea. Patient ECG is shown below.
ECG during tachycardia (Click on the image to enlarge it)
") |
ECG during tachycardia (Click on the image to enlarge it)

Description of the ECG-Regular tachycardia at heart rate around 200 per minute, right axis deviation, QRS duration 120 msec, no capture beats, no fusion beats, no visible P wave seen, so we can say it is relatively broad complex tachycardia although QRS duration is not fulfilling all the criteria for Broad complex tachycardia. So the differential could be Ventricular tachycardia or supraventricular tachycardia with aberrancy.
Patient underwent cardioversion. Post cardioversion ECG is shown below.
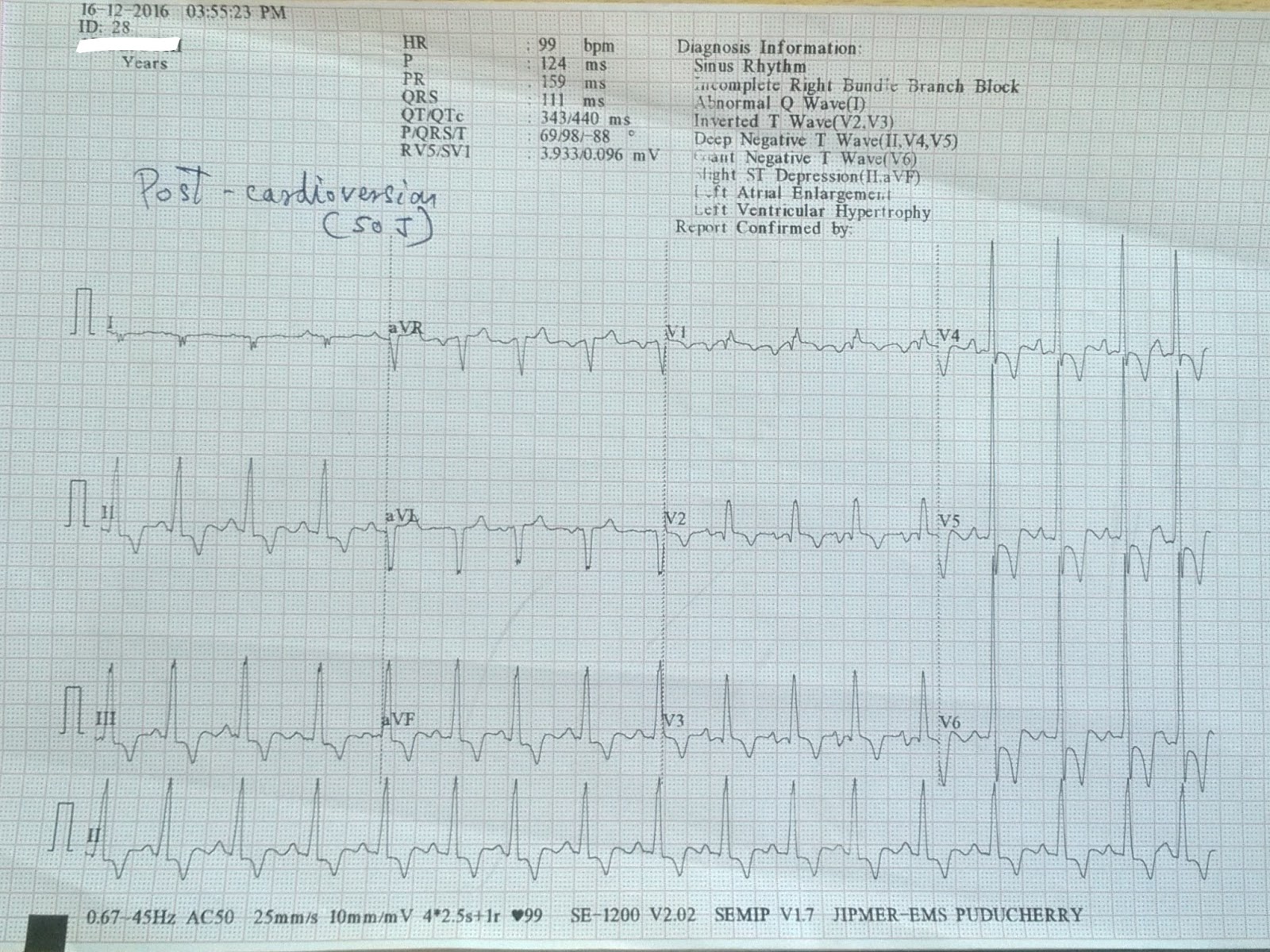
So the above patient post cardioversion ECG is similar to ECG during tachycardia. Patient post cardioversion ECG is also showing RBBB pattern, which favour the diagnosis of Supraventricular tachycardia with aberrant ventricular conduction.
How to approach in a patient with Broad complex tachycardia


No comments:
Post a Comment